Mastering Foot Anatomy : Infant vs Adult Feet & Growth Stages
Reading Time: 8 – 9 minutes
Continuing our Mastering Foot Anatomy series from Mastering Foot Anatomy: Foot Arches, Skin, Sweat Glands and Foot Types Explained, we now explore the remarkable transformation from infant to adult feet. This journey spans over a decade and involves dramatic changes in structure, function, and resilience. For parents, caregivers, pediatricians, and professional shoe fitters, understanding these shifts is non-negotiable—it directly impacts posture, gait, and lifelong foot health..
Foot Anatomy of Infants vs. Adult Feet
Development of the Infant Foot
A newborn’s foot is deceptively complex. At birth, it contains all 26 bones that will eventually form the adult foot—but most exist as soft, pliable cartilage. These cartilaginous precursors are separated by wide growth plates (epiphyseal plates), allowing rapid expansion. The heel bone (calcaneus) and metatarsal heads are among the first to begin ossification, but the navicular bone—critical for arch formation—remains cartilaginous until age 3–5.
The foot appears flat, wide, and pudgy, with a thick fat pad concealing the underlying structure. This fat pad serves dual purposes: shock absorption during early weight-bearing and protection for delicate tissues. By age 2, this pad begins to thin, revealing the emerging arch.
Pro Tip: Never force a baby’s foot into stiff shoes before 12 months. Barefoot time on safe surfaces builds natural strength and sensory feedback.

Natural Acrobatic Character of Infant’s Foot
Evolutionarily, human infants retain primate-like foot dexterity. The big toe is slightly abducted (angled outward), and all toes are longer proportionally than in adults. Most remarkably, infant toe flexors generate 10–15 times more grip force per gram of muscle than adult equivalents. This allows babies to grasp objects, stabilize during tummy time, and even climb (with support) long before walking.
This “hand-like foot” phase peaks around 6–9 months, coinciding with increased mobility. As ossification progresses, this grip strength gradually diminishes to prevent interference with efficient walking mechanics.
Pro Tip: Let babies go barefoot or wear soft-soled booties to encourage toe splay and grip development. Avoid rigid pre-walkers—they restrict natural movement.


The 5 Growing-Up Stages to Walking
Motor development follows a predictable sequence, each stage reshaping foot function:
- Sitting Up (4–6 months) – Toes curl reflexively for balance; plantar grasp reflex dominant
- Creeping (7–9 months) – Push-off strength develops in metatarsals; knees drive propulsion
- Standing with Support (9–11 months) – Weight shifts to heels; fat pad compresses under load
- First Steps (11–15 months) – Wide base, high guard arms, outward foot rotation for stability
- Active Walking (15–24 months) – Narrow stance, arms at sides, heel-to-toe roll emerges
Each transition strengthens specific muscle groups and accelerates bone remodeling in response to mechanical stress (Wolff’s Law).
Pro Tip: Avoid walkers or bouncers that force upright posture too early—they can delay natural muscle development and increase fall risk

First Steps: How Infants Balance
The neuromuscular learning curve is steep. At 11 months, the center of mass is high (near the chest), requiring a wide base of support and elevated arms for counterbalance. Feet often turn outward (external tibial torsion) to widen stability.
By 15–18 months, the pelvis widens, core strength improves, and the child adopts a mature gait pattern: arms swing reciprocally, feet point forward, and step length increases. This shift reflects myelination of neural pathways and ossification of the tibial tuberosity.
Pro Tip: X-rays are rarely needed—regular shoe size checks every 6–8 weeks are the best growth monitor. Sudden jumps (e.g., 2 sizes in 3 months) are normal during puberty..



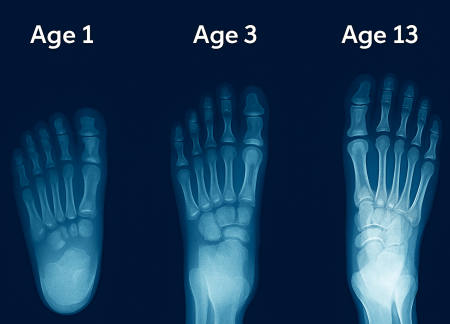
Progressive Bone Development
Ossification is not linear—it accelerates during growth spurts:
| Age | Key Ossification Events |
|---|---|
| 0–1 year | Calcaneus, talus, cuboid begin hardening |
| 2–3 years | Metatarsal heads ossify; fat pad thins |
| 4–6 years | Cuneiforms solidify; medial arch emerges |
| 8–10 years | Navicular fully ossifies; longitudinal arch matures |
| 12–14 years | Growth plates close; adult proportions achieved |
By age 13, the foot reaches 90–95% of adult length, but width and arch height continue refining until 16–18.
Pro Tip: Use non-slip socks or barefoot walking on carpet to build proprioception (body awareness). Avoid slippery floors during this phase.
Signs of Trouble vs. Healthy Development
| Warning Signs | Healthy Milestones |
|---|---|
| Persistent toe walking after 24 months | Sits with feet flat |
| Severe in-toeing/out-toeing | Feet align forward by 18 months |
| Pain or limping | Confident, pain-free gait |
| Asymmetrical shoe wear | Even wear patterns |
| Flat feet persisting past age 6 | Visible arch by age 5–6 |
Pro Tip: If your child complains of foot pain or refuses to walk, consult a pediatric podiatrist immediately—early intervention prevents lifelong issues like bunions or plantar fasciitis.
Key Differences: Infant vs. Adult Foot (Summary Table)
| Feature | Infant Foot (0–2 yrs) | Adult Foot |
|---|---|---|
| Bone Structure | 90% cartilage, wide growth plates | Fully ossified, fused joints |
| Arch | Absent (fat pad conceals) | Longitudinal + transverse arches |
| Toe Grip Strength | 10–15× adult level | Minimal (used only in balance sports) |
| Fat Pad | Thick, protective layer | Thin, localized under heel/metatarsals |
| Flexibility | Hyper-mobile, “hand-like” | Rigid, lever for propulsion |
| Growth Rate | Up to ½ size every 2 months | None after ~16–18 years |
| Shoe Needs | Soft, wide, flexible | Structured support, cushioning |
Conclusion: Why This Matters for Shoe Fit & Comfort
Children’s feet are biological construction sites. A shoe that fits in June may cause blisters by August. Follow the Golden Rules of Pediatric Fitting:
- Check every 6–8 weeks until age 5, then every 3–4 months
- ½ inch growing room (thumb width at toe)
- Flexible sole that bends at the ball of the foot
- Wide, rounded toe box to allow full splay
- Secure heel counter to prevent slippage
Pro Tip: Mark your calendar! Set a “shoe check” reminder every 2 months for kids under 5. Use the “thumb test” at the toe and “pinkie test” at the heel.
Next Blog: Foot Dynamics – Foot Motions, Weight Bearing…